BREAST POSITIONING DEVICE FOR PATIENTS WITH LARGE BREASTS UNDERGOING RADIATION THERAPY
Gunilla C. Bentel, RN, RTT
Duke University Medical Center
Durham, North Carolina
INTRODUCTION
Several studies have shown that local excision followed by radiation therapy in the management of early stage breast carcinoma yields results that are similar to that of a radical mastectomy.1,4,6,7
An increasing number of patients are therefore electing local excision followed by radiation therapy in the management of their disease. A small percentage of these patients present with large/flaccid breasts that, from a technical standpoint, is difficult to treat. In a few patients, these difficulties may be so severe that a mastectomy is recommended. Some radiation oncologists may be reluctant to treat patients with large breasts due to the possibility of poor cosmetic result.5
A large heavy breast tends to migrate cephalad when the patient is in the supine position or it may droop laterally (Fig. 1). When the breast is too far cephalad, the tangential beams across the chestwall may not clear the arm and in patients where the breast is on the lateral chestwall, the lung volume within the tangential fields may be excessive.

Fig. 1 Large/flaccid breasts tend to droop laterally. Set-up mark, indicated by the arrow, represent just one of many that are made on the Alpha Cradle®* device. Also, note the handle which the patient is holding onto.
*Registered by Smithers Medical Products, Inc.
Attempts to cause a caudal gravitational shift of the breast by elevating the patient’s shoulders on a slanted board frequently fail because the position is difficult to maintain. In some patients, skin folds may also form between the breast tissue and the skin surface of the upper abdomen and in patients with large pendulous breasts, the tangential fields must be extended farther caudal than is customary, hence including more normal tissue. Treating the patient with a brassiere in place has also been tried, however this precludes set up marks from being made on the patient’s chest. A brassiere also frequently moves the opposite breast closer to the tangential beams and may compromise the needed beam angles. A stockinette around the chest to hold the breast in place tends to compress the breast tissue and thus spreading the volume of breast tissue over a larger area of the chestwall. The tangential fields may then need to be enlarged hence, more normal tissues are irradiated. Skin folds are also more likely to be caused by this compression method.
Dose inhomogeneity within the breast and chestwall in patients with large breasts presents another area of concern, however, the ability to position the breast in a more advantageous location on the chestwall may address this issue in some patients.
POSITIONING DEVICE
The patients are positioned supine in a half-body ALPHA CRADLE®* device described in a later report, (see Immobilization Device for Patients Undergoing Radiation Therapy for Carcinoma of the Breast, page 47), with the ipsilateral arm elevated.² The breast positioning device,³ the Bravelle™, which is quite simple to use, consists of a reinforced polyvinyl chloride (PVC) tube with an outer diameter of 7/16”. The length of the tube is cut to loosely fit around the circumference of the base of the breast. A polyethylene barbed fitting is used to close the two ends so that the tube forms a ring. The ring is placed around the base of the breast and a Velcro® tape, 40-50” long and placed under the patient’s chest, is attached to each side of the ring. The breast is then manually moved into the appropriate position and the Velcro® tape is tightened so the breast remains in the desired position (Fig. 2A and 2B). The Velcro® strap is placed “under” the opposite breast within the inframammary fold in an effort to pull the involved breast caudal.

Fig. 2A The breast ring helps to move and maintain the breast in a more advantageous position during radiation therapy.

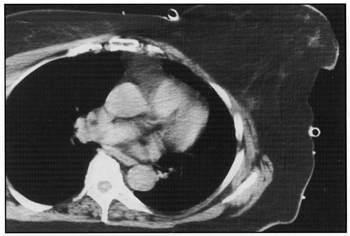
Fig. 2B In some patients, the breast tissue will assume a mushroom-like shape causing a skin fold between the breast and the chest. The computed tomography images illustrate the breast position with and without the breast ring in place. In this very obese patient, with a thick chest wall, the volume of lung tissue within the tangential fields was not changed by the use of the breast ring. However, it was difficult to determine the lateral extent of the breast tissue and by moving the breast anteriorly, it was felt that the margins were adequate.
In some patients with large/flaccid breasts, the breast tissue may assume a mushroom-like shape over the ring (Fig. 2A). A 2” high circle or semicircle of Styrofoam®*, is taped to the breast ring as a retaining wall for the breast tissue (Fig. 3A and 3B). A skin fold will sometimes form between the breast tissue and the chest, particularly in the inframammary fold. To prevent loss of skin sparing in the folds, a piece of Styrofoam® is placed in the crease between the tissues so they become separated (Fig. 3A).
* Registered by Dow Chemical

Fig. 3A A “retaining wall” taped to the breast device and a Styrofoam wedge used to prevent skin folds…

Fig. 3B With the “retaining wall” in place, the breast tissue is moved anteriorly.
Set-up marks are made on the skin peripheral to the breast itself and on the ALPHA CRADLE® device. The sagittal alignment line is marked caudal to the inframammary fold on the upper abdomen and in the supraclavicular region extending onto the ALPHA CRADLE® device. The transverse alignment line and the medial and lateral fields are marked on the presternal skin, the lateral aspect of the chest, and on the ALPHA CRADLE® form. Internal mammary and supraclavicular fields are matched in the usual fashion.
RESULTS
The device has been used in 18 patients in our department. In the majority of these patients, the goal has been to move the breast from the lateral chest wall to an anterior position. When the breast was moved more anteriorly, the lateral field margin could, in some patients, also be moved more anterior, thus the volume of lung tissue within the tangential fields was reduced. In some patients, the shift of the breast position was in more than one direction and in one patient the breast was shifted cephalad.
Another benefit of repositioning the breast from the lateral to medial position is the improved dose uniformity across the breast and chest wall, which occur when the breast is positioned closer to the midpoint between the medial and lateral entrance point of the tangential fields.
All of the patients treated using the breast ring have developed small areas of moist desquamation in the inframammary fold, which healed soon after completion of therapy. One can surmise that had these patients been treated without raising the breast, the skin reaction might have been more severe. The cosmetic result, recognizing the short follow up (1-29 month), has been excellent.
DISCUSSION
Irradiation of patients with large breasts is technically very difficult and some radiation oncologists hesitate to treat these patients due to the risks of poor cosmetics result. The device described in the report, the Bravelle™, manufactured by Smithers Medical Products, Inc., has made it possible to treat breast cancer patients who otherwise would not be candidates for radiation therapy due to the enormous technical difficulties they present. The reproducibility of the breast position has been satisfactory and no adverse reactions have been observed in 18 patients that have completed radiation therapy using this device.