ALPHA CRADLE® HS3 THORACIC MODIFICATION FOR BREAST & CHEST WALL PATIENTS
Max Buscher
Tufts New England Medical Center
Boston, Massachusetts
The majority of patients needing breast or chest wall irradiation are treated with opposing tangential photon fields. The problem of the sloping chest can be solved by collimator rotation or an angled breast board.
Collimator rotations of greater than 3° can lead to unacceptable large divergence into the anterior Hockey Stick or supraclavicular fields. This department prefers to angle the patient’s thorax upward to eliminate the slope, i.e., the chest is made horizontal over the length of the tangential fields.
We have tried various adjustable-angle breast boards and found them unsatisfactory for two reasons. These devices are heavy and cumbersome, as they need to be rigid enough not to sag. This requires they be made from a strong material (wood and plastic have been tried). Secondly, they failed to reproduce the patient’s neck extension and shoulder and arm position.
A customized and angled immobilizer can be made by modifying the ALPHA CRADLE® brand HS3 device. The shell of this form is shown in Fig. 1 and the inside piece is shown in Fig. 2. It is from this usually discarded inside piece that in inclined plane is assembled.
This piece is cut into four sections (Fig. 3) using a hot wire cutter. First the head section is cut off and this is then sliced in half length-wise. One half is discarded. The remaining right and left side pieces are each cut diagonally, from top to bottom, to form the right and left sections of an inclined plane.
Notice that two holes (actually “bites”) are cut in each of the pieces to accommodate the pouring of the chemical – at the shoulders and near the ribs. There will be two pieces left over – the two right and left “tops”. One is discarded and the other is trimmed slightly so it can form the middle section of the inclined plane.
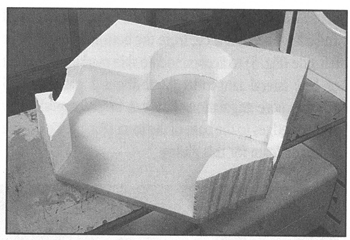
Fig. 4 shows these pieces assembled into the shell. The three pieces that form the inclined plane should be taped in at the bottom to prevent shifting and leaks. The chemical is poured into the four holes already cut and into the head section. About 1/3 of the chemical should be used in the head area. The whole form is then draped with a mylar sheet and the patient is laid back into it and positioned.

Fig. 1 The HS3 shell

Fig. 2 The inside piece.

Fig. 3 The inside piece modified
When the urethane hardens the mylar is stripped off and a large section is cut from the bottom of the right or left side (Fig. 5) to accommodate skin marking the (right of left) lateral tangential field. About 1 patient in 15 requires more angulation. This can be accomplished by gluing wedges to the base of the form (Fig. 6). We use the urethane foam for this gluing.

Fig. 4 The pieces assembled back into the shell.

Fig. 5 The poured and finished product.

Fig. 6 Wedges added for extra angulation.
The cutting preparation described her takes less than ten minutes. We have been using this modified HS3 immobilizer for five years. It is light and provides adequate thorax angulation. It reproduces head position, neck extension and arm position. It has also proven to reduce set up times on the treatment machine.